Current Treatment Challenges
Many factors complicate treatment decisions in R/R PCNSL
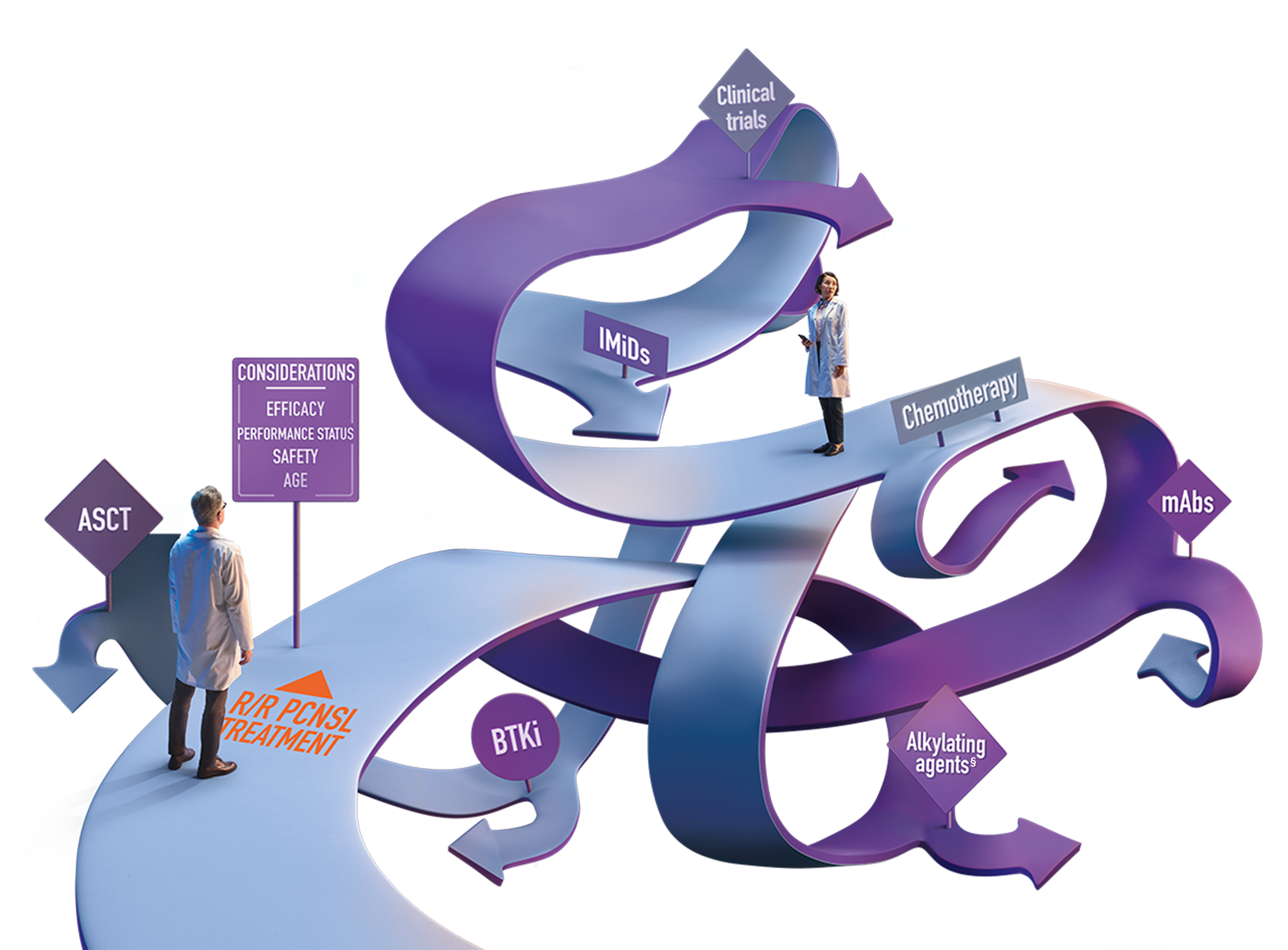
Many factors must be weighed when choosing a treatment
PCNSL relapse may occur at different intervals, with early/short relapse (<12 months from treatment initiation) distinct from primary refractory disease1,2*
Considerations include3:
Patients may be unable to receive further intensive therapy due to multiple factors3-6
- Advanced age
- Impaired performance status
- Poor physiological fitness
- Debilitating symptoms, such as cognitive impairment and paralysis
- Renal, lung, bone marrow, and cardiac function
- Tolerability of initial treatment
- Other comorbidities
The availability of caregiver support and a patient's ability to travel for care may impact treatment decisions
Many patients with R/R PCNSL are ineligible for further intensive treatment, such as HD-MTX1-3*
Factors that impair the ability to receive HD-MTX include7:
Additional current treatments
For patients who relapse or are refractory following first-line PCNSL treatment, additional options that may be considered include HDC-ASCT, WBRT, or other single-agent and combination regimens.8

Additional regimens, including targeted and immune-based therapies, have been studied in R/R PCNSL clinical trials as single agents or in combination4,8,14
In general, use of novel agents is recommended within the context of clinical trials8
There are limited FDA-approved options for R/R PCNSL3,4,10
The management of patients with R/R PCNSL remains poorly defined and is a major area of unmet clinical need15
- Although the treatment of PCNSL has evolved during the past few decades, there is no accepted standard of care in R/R PCNSL16
Many regimens have been studied; however, there are limited FDA-approved therapies for R/R PCNSL3,8,10
As a result, treatment approaches vary6,15:
- Chemotherapy: HD-MTX rechallenge, other chemotherapy regimens
- HDC-ASCT
- WBRT
- Targeted agents and immunomodulatory approaches
- Clinical trials
There is no clear choice in treatment options for the management of R/R PCNSL8
Want more information about R/R PCNSL?